[soundcloud url=”https://api.soundcloud.com/tracks/174118161″]
Videos by Rare
Kurt Wallace: This is Kurt Wallace, and our guest today on Rare is David Newberry. He served 25 years with CDC’s infectious disease unit to help eradicate smallpox, initiated President Carter’s guinea worm eradication project in Ghana, and served as a consultant with both Johns Hopkins University’s Department of International Health and with the U.S. government. He has first-hand experience in three disease eradication programs: smallpox, guinea worm, and polio. And, David Newberry, with that kind of a resume– thanks for joining us today on Rare.
David Newberry: It’s my pleasure, Kurt. Thank you very much for asking me.
Kurt Wallace: Well, we appreciate you coming on today. Let’s go ahead and talk about what’s going on with the Ebola situation. First off, what is the role of an epidemiologist at the CDC?
David Newberry: Well, epidemiology comes — the term itself comes from three great words: epi — a form like epidermis, and then demo — the people, and then ology — the study of. So, it’s the study of diseases that come on the people. So, it’s like being a medical detective sometimes, Kurt.
Kurt Wallace: When we talk about the Ebola virus, when did you become concerned about how the CDC is handling the Ebola virus?
David Newberry: Well, the concern is — back in April, several of us that had served overseas for many years and had some experience with the Marburg Lassa fever and the Ebola virus were concerned that we weren’t really looking at ways of dealing with it in countries that were infected — very complex West African countries that were infected.
So, we were trying to generate at least a cadre of us old-timers that had worked out there and lived out there to initiate a sort of early surveillance system — one that would give us an idea of the dimension of the problem.
Our concern was raised, Kurt, on the basis of actual reported cases occurring because, usually, the outbreaks preceding this had a few cases. But, then this dimension of this was kind of scary because it was actually getting into the official system.
So, we were pretty sure there was going to be kind of a big outbreak. But, it was hard to find a voice, and most of us old-timers were kind of left in the dust with all the new prestige stuff.
The amount of money that’s being generated is, also, a trap because people think about money and prestige and that sort of thing. So, we didn’t get a good hearing, but maybe we just didn’t make the appeal very well. I don’t know.
Kurt Wallace: Well, let’s talk about the nature of Ebola. I understand there are five separate strains of the virus?
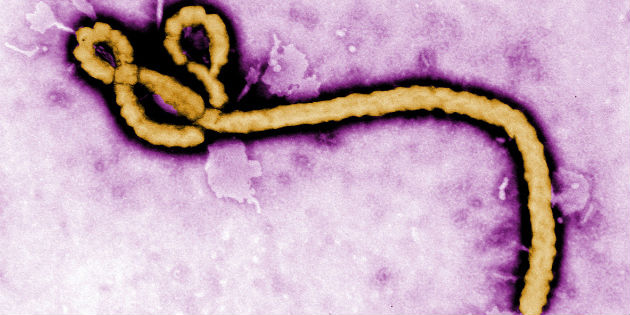
David Newberry: Right, it’s a Filoviridae virus — hemorrhagic fever kind of virus. And, hemorrhagic fevers, by description, are very scary because they cause bleeding, and they have a fairly high mortality rate — hard to treat — and people become infected dealing with the treatment aspect. It’s also scary in the sense that we look at it being a disease that has a very long incubation period. When we looked at five strains emerging — only the Reston version doesn’t bother humans — the other four do. You look at the emerging knowledge that we have on it — the fact is, we have five strains that can mutate fairly easy. And, our fear and concern would be: is it possible that this may mutate into an airborne virus? If it is, then, we’re sort of back in the Middle Ages. But, again, that is only a concern — that we would think about — as we look at the number that have already mutated.
Kurt Wallace: So, the possibility of Ebola actually mutating to an airborne virus and becoming a serious pandemic is real?
David Newberry: Well, it’s possible. Yeah, it’s possible. You know, back in ’75 we had the pandemic of Cholera that swept around, and it took an enormous amount of international public health work and endeavor to eliminate that or bring it under control. We did.
If you look at the current situation — I think there are a little over 9,000 cases with about half of those dying, with about 4,500 deaths — it’s nothing to monkey with. And, again, speaking of monkeys, that’s part of the problem. We have considered that there is a zoonotic connection between fruit bats and, perhaps, primates — which are also dying from Ebola.
So, again the mechanism of transmission by direct body fluids — and looking at the zoonotic connection in these infected countries in West Africa — makes us very leery about what we can do, and how we can stop it, and how we can control it.
And, early detection and quarantine looks to be the most favorable mechanisms. But, then you look at the number of health care workers that have contracted and died from Ebola just taking care of other patients. I mean it makes a very dismal outlook in terms of our own personal efforts — in terms of public health efforts. Everybody’s got to work on it.
Kurt Wallace: At this point, with Ebola the way it is in Africa — is there concern of a major outbreak in the United States?
David Newberry: I’d say concern is always there. Yes, that’s what public health is about and the world has become a shrinking globe with the ability of people to move trans-globally in a few hours. So, the potential is there, but I think the idea of early detection — and Hopkins just held a seminar looking at five questions: What’s Hopkins doing to ensure its patients and visitors are protected? How do doctors and healthcare workers stay protected? If you have virus symptoms, how contagious is Ebola? Those are the five major questions of the seminar.
But basically, it’s early detection and proper hygienic and protective clothing use. And, we’ve always been able to use ordinary protective garments in the hospital situation to protect people.
But, Ebola is tricky because the traditional garments don’t appear to be 100% in preventing the transmission of the virus. Because all you need is three things, Kurt, for transmission: a susceptible individual, an agent that causes illness, and a means of transmission. And, we look at the patient care — transmission rate is very high. And, the reason that is, is because when you put that protective clothing on — if it gets wet and you monkey with that — and that wet product or fabric can be the means of transmission.
So, we need to look at ways – and, they are getting into the space suit, the real esoteric kind of protective garments for healthcare workers. Survival depends on good health care and, of course, as we know we lose about half the patients anyhow.
So, this means of garbing the protective clothing and protective gear and disrobing that has caused healthcare workers to – and, we had this lady in Nigeria, all she did was to take the glove off, her protective glove off — to remove the I.V. from a patient that had just died — and that was enough. The idea of just common ordinary means to protect yourself from infected disease has to be strengthened and has to be rigorously practiced.
Kurt Wallace: In terms of contracting Ebola from other people. Can it live outside the body? How long does it hold in the body in different areas, different fluids?
David Newberry: Well, the research is still ongoing, but we’re advised that the male may carry Ebola virus in the semen for up to seven weeks. So, recovering male patients are advised to refrain from sexual activity that isn’t protected. And, of course, we know that breast milk can transmit the virus as well. And, then, there’s also the possibility, albeit remote, that if you have the aqueous chamber of the eye, also, retains the Ebola virus for fairly — nobody knows exactly how long. So, it’s present in three areas: the semen of the male, the breast milk of the mother, and the aqueous chamber of the eye.
And, this is ongoing research. That’s just what we’re advised of at the present.
Kurt Wallace: Let’s talk about neighboring countries to the United States — countries around the world that have actually had cases of Ebola. We have undocumented workers that are crossing over the border from Mexico to the United States. What are we looking at?
David Newberry: Well, we’re looking at countries that have had initial cases or localized transmission. And, then Nigeria, of course, had 19 confirmed cases. Well, they had actually one probable as well — so they had 20 — and eight of those died.
Senegal had one case confirmed and survived. Spain had one case and survived. The United States had three cases and one death. So, you’re looking at the total aggregate of localized transmission countries that the total case number is 25, and of those 25 — nine have died. We would say that they had probably much better medical care than you’d get in Liberia or one of the other West African countries.
Kurt Wallace: Are there concerns about Mexico’s capabilities?
David Newberry: Obviously, the borders are pretty open. If Ebola appears in Mexico, then I think we can really look at a panic.
Kurt Wallace: What are some things people can do on their own volition that could possibly help contain Ebola? There are people that are concerned about — the CDC is not doing enough. As a libertarian myself, I never believe that government is that capable of taking care of the things that individuals can also do and need to do to take care of themselves. In this case, what are some things people can do?
David Newberry: Well, first of all you can go online and buy a trick to survive Ebola. You can buy it for seven dollars, I think. People, entrepreneurs, are always making money off this sort of thing.
But, in answer to your question – obviously, good person hygiene and moderate amount of care. Because flu season is also coming, so it will be very difficult to differentiate between flu and more serious illness. I tell you what I would do. I would take — there are West African country residents that are legal residents of the United States. And, the people moving back and forth from these infected countries; they are here in social — they have church and social communities from Liberia, Monrovia and different places. And so, I think, I would recruit these folks and train them about early detection and have them help monitor people that are travelling back and forth. And, teach them that you need to be very careful about your personal hygiene behavior.
I think that if we had an early detection system comprised of people who were in contact with these folks that travel from these endemic areas; I think that would give us a leg up on being able to identify someone who might be — might have been exposed in monitoring that person.
And, it has a long incubation period, Kurt. It’s got a 21 day incubation period and the mean is eight to 10 days. But, standing in the airport with somebody that’s been exposed 10 days ago and has no sign or symptom is not really going to issue the problem.
And, then the government’s responsibility to protect healthcare workers is the next greatest feat we have. They need to get the space-age equipment out to these hospitals and perhaps generate a rigorous training program on: how to robe, and how to disrobe, and how to maintain the integrity of their protection against an individual patient. That’s all common sense; but again, I think the responsibility is going to fall on the people themselves — particularly in healthcare facilities themselves, I think, if we have a significant number of cases that come in.
Kurt Wallace: David Newberry 25 years with the CDC. You’ve done a lot of work. Thank you for the work that you’ve done and thank you for spending time with us today on Rare.
David Newberry: It’s my pleasure, Kurt, I really appreciate the opportunity and wish you and America — God bless America — against this virus.